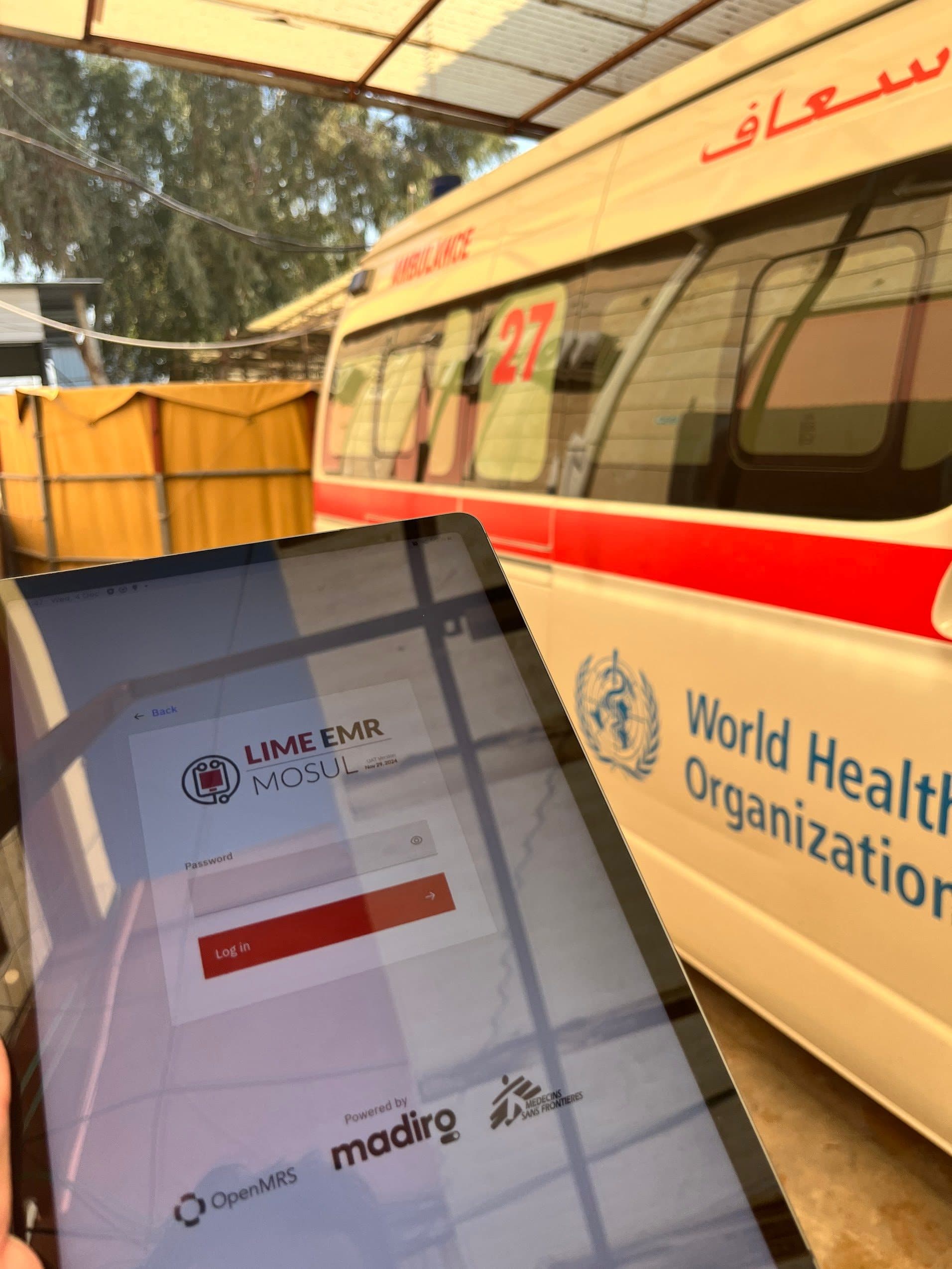
Continuity of care.Continuity of data.
We help humanitarian and global health organizations get through innovation and transformation — from deploying clinical systems to training local teams to own them.
Solution ready in days, not months, at a fraction of traditional implementation cost and using open standards.
Trusted by humanitarian orgs, Ministries of Health, and global health programs

The tools are deployed. The data still isn't flowing.
Every week, your teams work around systems that should work for them. The data exists — but it can't be found, compared, or trusted.
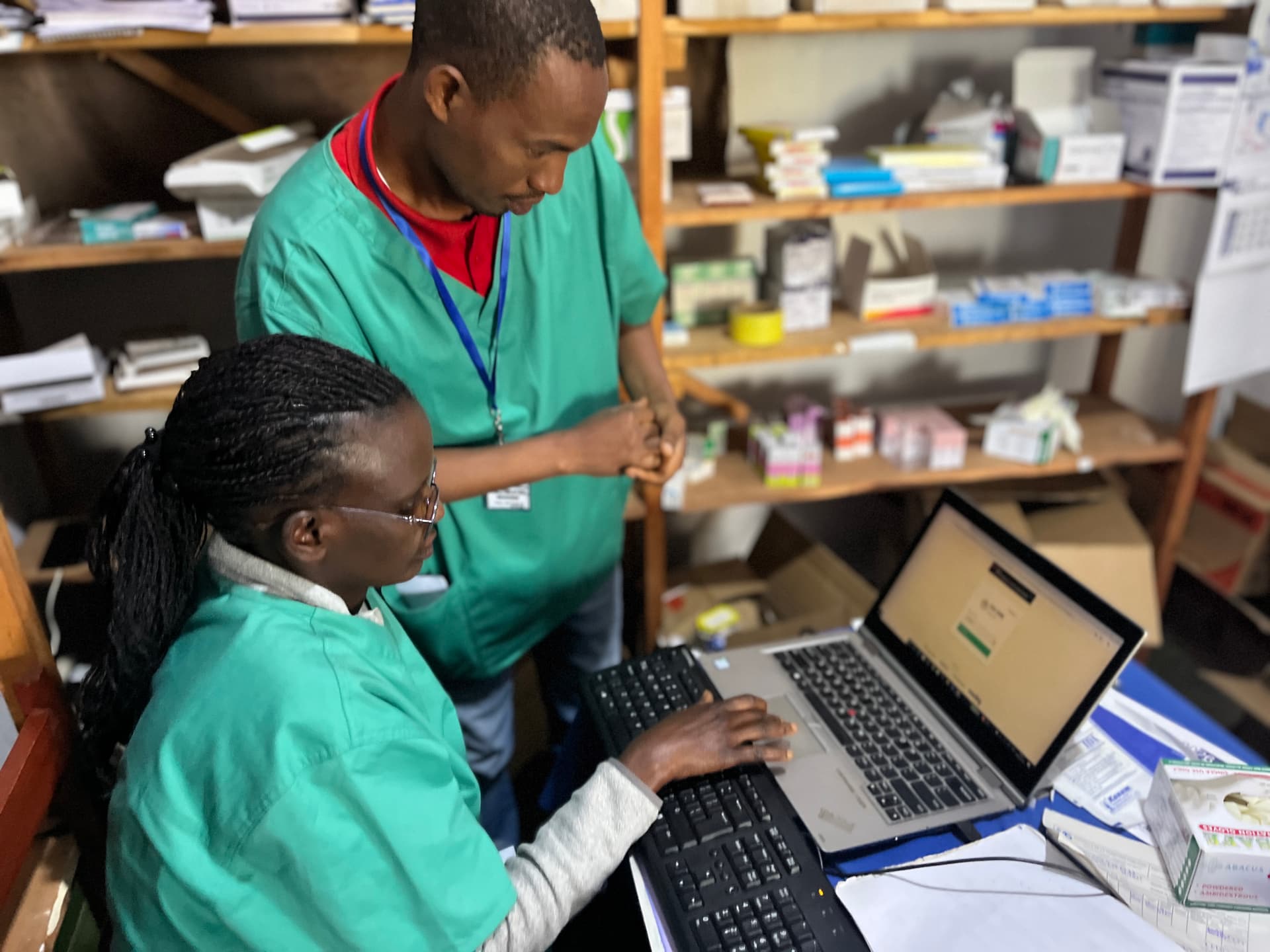
A patient is seen. The report is still done by hand.
Your clinical system and your reporting platform don't talk. Someone reconciles them manually — every week, every facility, every program.
New program. Weeks of waiting for a form.
Every new clinical protocol triggers the same backlog: concept mapping, form development, sign-off — before a single patient is seen.
Three teams. Three counts. Three different answers.
Without shared terminology, data can't be compared across sites or systems. Every export needs manual reconciliation before it can be used — or trusted.
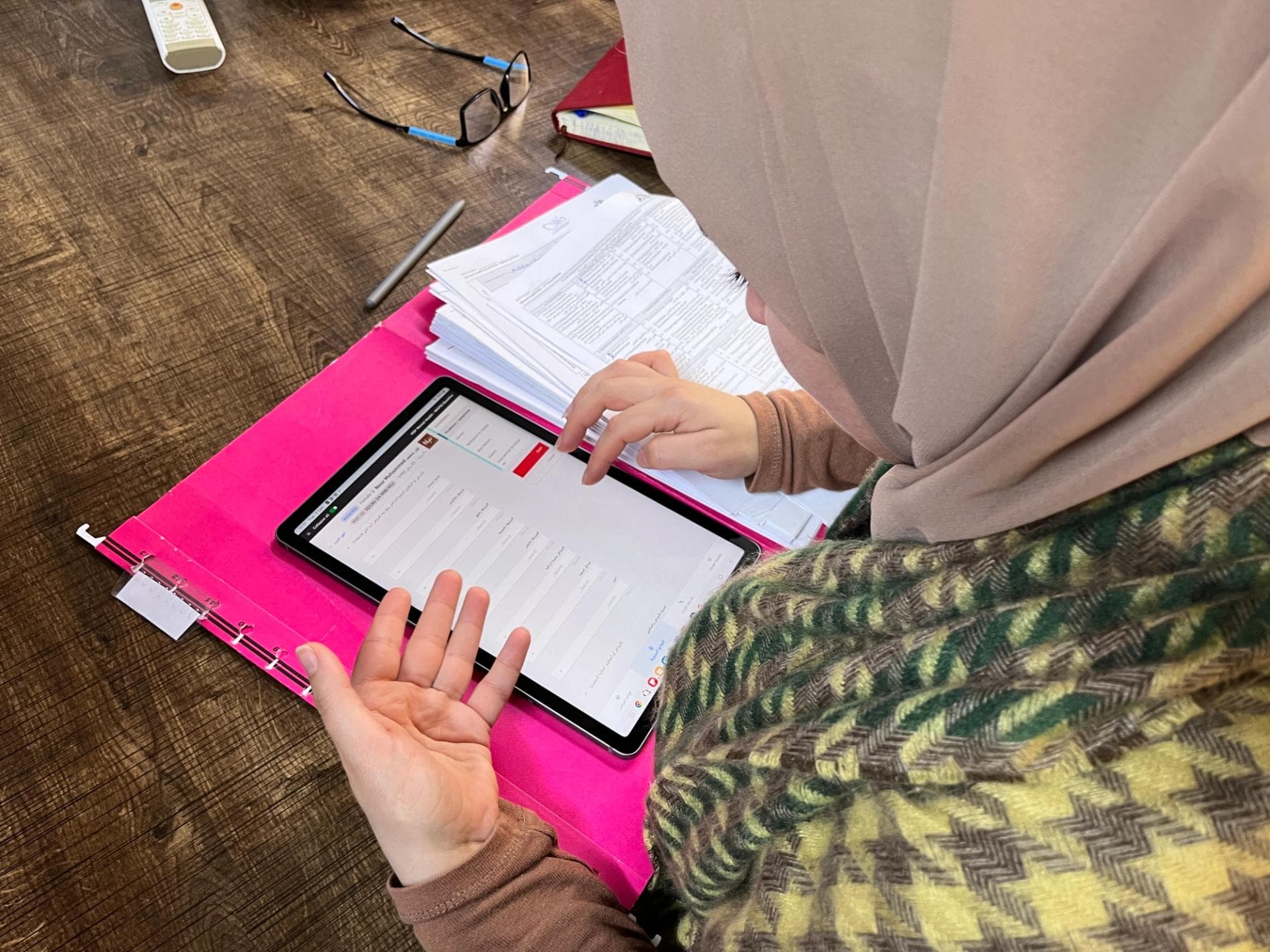
Care happens offline. Data stays there.
Community health workers reach patients no system ever captures. Paper forms, days of lag, data entered late — or never. The patient has already moved on.
The system works. Until the vendor leaves.
Tools get deployed. Donors move on. Local teams inherit systems they weren't trained to own, can't troubleshoot, and can't adapt. The paper forms come back.
Built to last
without us.
Every principle here is a direct response to how digital health implementations fail — and a deliberate design choice to prevent it happening again.




Built once. Reusable everywhere.
Every tool we use — OpenMRS, DHIS2, OpenFn, FHIR — is open-source and community-maintained. We contribute 70+ clinical forms across 12+ health programs back to the global commons. Adding a new country is a mapping exercise, not a software project. Your investment doesn't stay locked in one program — it becomes infrastructure that every similar program inherits.
AI-agentic pipelines. From data to decision.
Clinical forms, interoperability mappings, GIS disease layers, supply chain forecasts — all built and tested through AI-assisted workflows designed by domain experts. New protocols go live in days, not months. Every AI step is transparent and auditable: epidemiologist review, ministry approval, full audit trail. Your team owns the outcomes.
Any system. Any language. All connected.
We build data pipelines that connect the systems you already have—whatever EMR, whatever national reporting system. Clinical terminology gets standardized across them using OCL and FHIR, following OpenHIE patterns. No more manual exports. No more spreadsheets. All data flows automatically and compares cleanly.
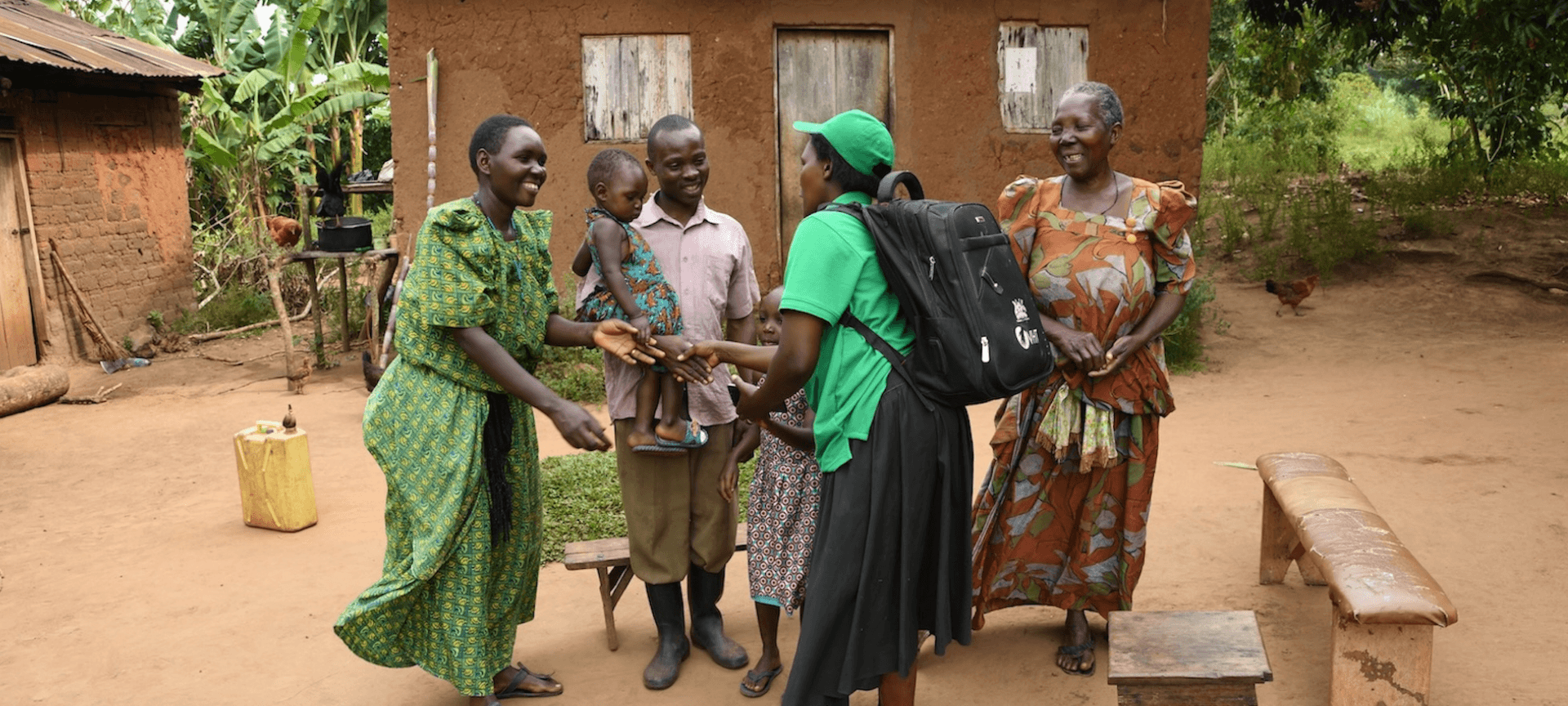
Offline Outreach. Syncs when back.
Full clinical workflows run offline — no internet required. Data stays in-country by default: local hosting, government-controlled servers, no foreign cloud dependency. A Ministry can terminate all external relationships and keep running. We also deploy field infrastructure that makes operations sustainable: solar power and satellite or cellular connectivity for eventual sync. When a signal is available, data flows automatically.
Global expertise. Local ownership.
We match digital health specialists from our global network to your specific context and health system. Every engagement is designed for knowledge transfer — co-building with local technical staff from day one so the system belongs to them, not to us.
We measure what we build.
We build monitoring frameworks aligned with log frames, WHO health system strengthening indicators, and USAID development hypotheses. We co-author implementation research with academic partners and publish findings in peer-reviewed literature. For humanitarian and climate-health programs, guessing isn't good enough — we measure, we publish, we adapt.
The challenge was real.
So are the results.
How we've solved health data challenges for organizations like yours.
Modular Health Records for Humanitarian Settings
Deployed to 3 countries in 75% less time. New clinical forms go live in under 5 days. Local teams now manage the platform independently — zero ongoing external support costs. Program budget reinvested into clinical expansion, not maintenance.
Offline-First Care & Field Infrastructure
Field teams now capture full clinical data offline with zero data loss. Solar and connectivity infrastructure extended coverage to remote sites. Patient documentation increased 40% across previously unreachable areas.

Complete Health Information System
Four integrated systems—EMR, pharmacy, billing, and analytics—all in the team's hands. Zero ongoing licensing costs. Zero external dependencies. Fully sustainable.

National Health Data Interoperability
National HIV program now has real-time visibility into facility data. Lab orders and results flow automatically. 20+ Ministry officials trained and fully in control — no external consultants, no licensing fees, no foreign cloud dependency. Supported through Data.Fi program funding.
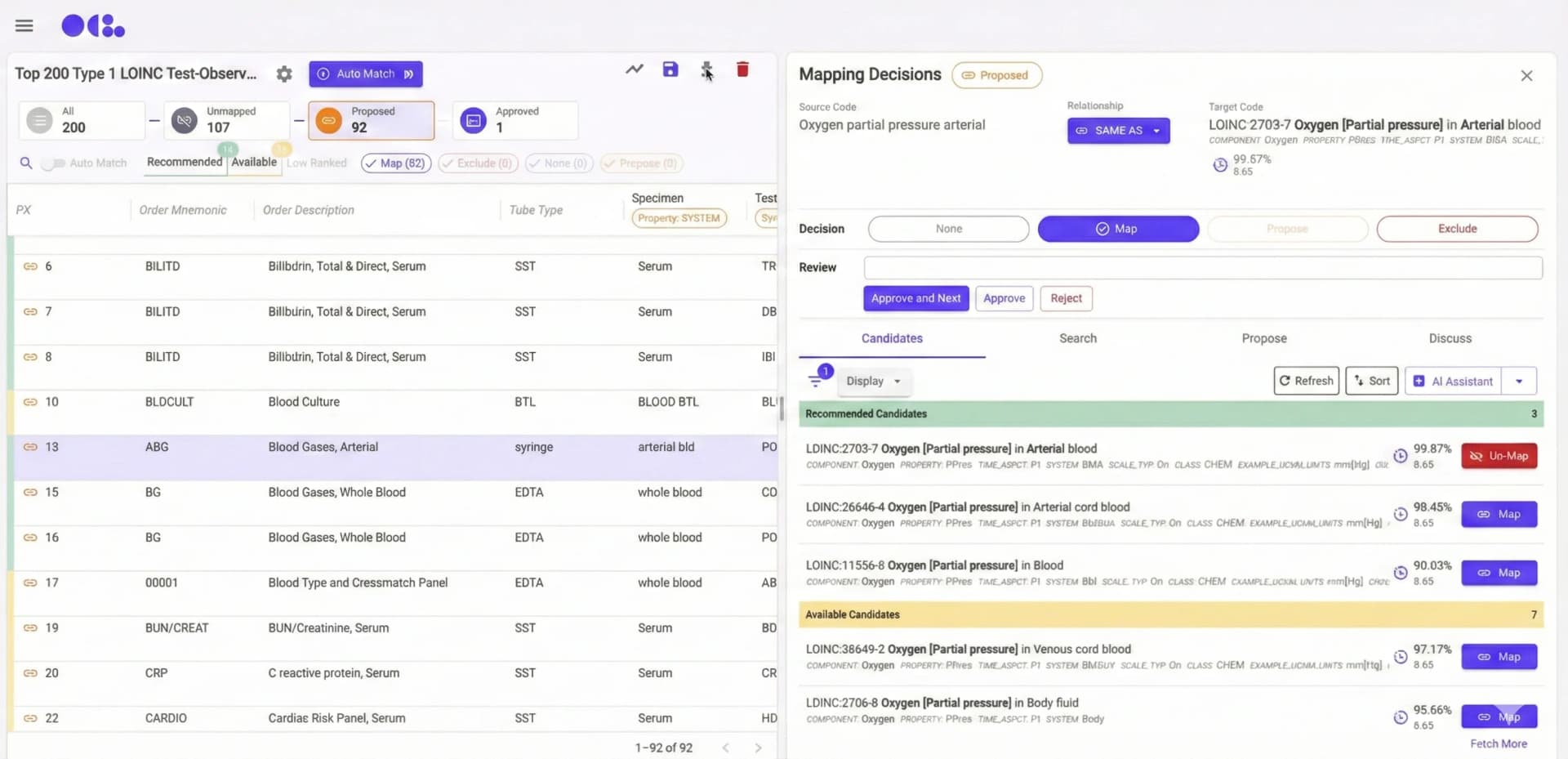
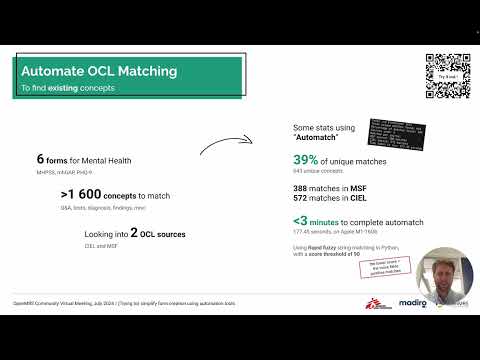
OCL AI Mapper: Automated Terminology Mapping
Terminology mapping across 55K+ CIEL concepts now happens dramatically faster. Domain experts focus on validation and edge cases—not routine mapping. Health programs launch weeks sooner.
M&E Framework & Evidence Generation
Active data collection across 3 districts covering 1,000+ households and 500 CHEs. Performance mapping integrates activity, GPS, and product sales data. CHE performance study submitted for peer-reviewed publication.
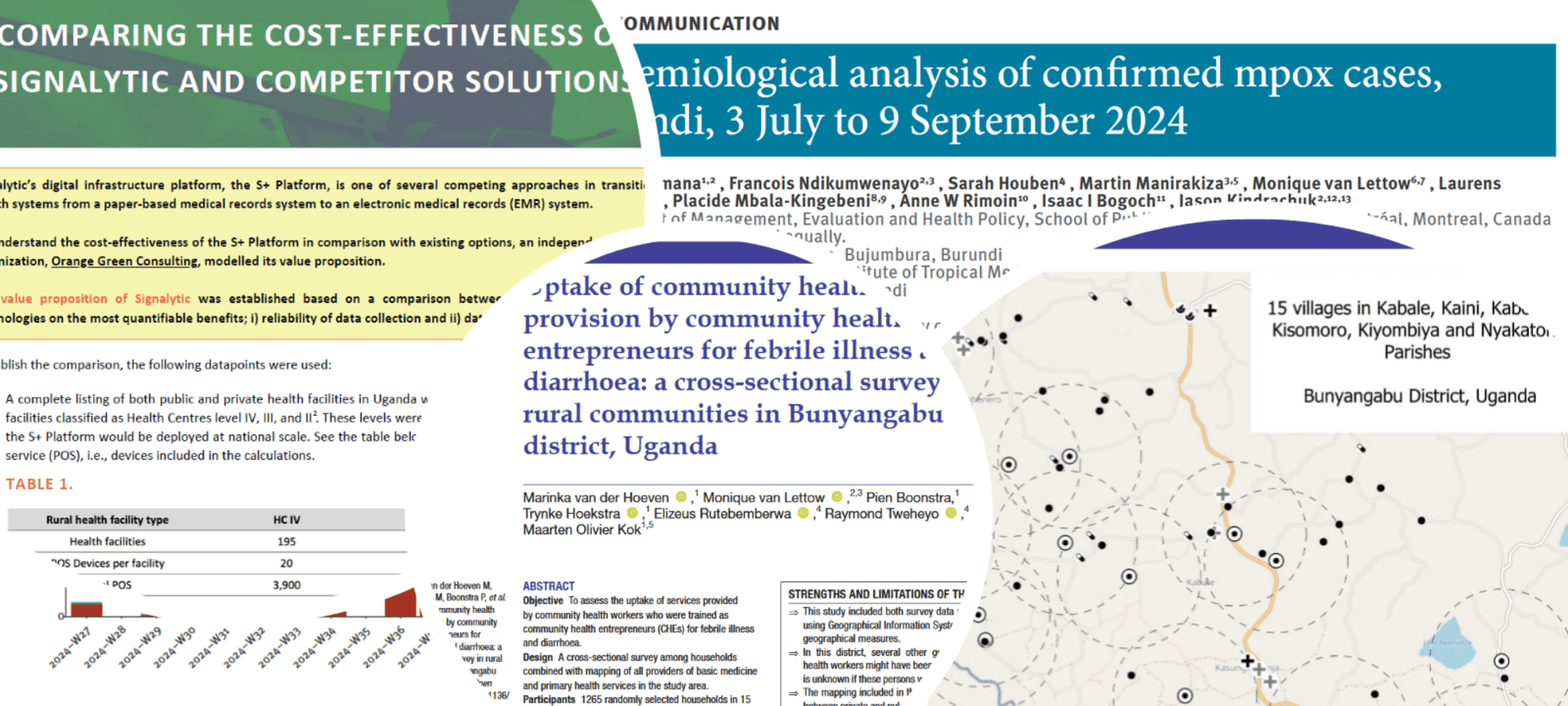
Research Development & Publication Support
Delivered 2 peer-reviewed publications, white papers on supply chain cost-effectiveness co-authored with MSF, and a qualitative study on mentorship models for African health start-ups—amplifying partners' global visibility.
Working on something similar? Let's talk.
Heard from the field.
Not from our website.
MSF, OpenMRS, and OpenConceptLab on what it actually looks like to build with us.
Through its philosophy and expertise, Madiro builds a bridge between the complex and evolving world of open source technologies, and the concrete reality of frontline MSF health workers in the field.

Madiro is positioned to be a catalyst, propelling our shared community vision to foster efficiency, reduce costs, and enable harmonious integration with national health systems.


Through our collaboration OCL has become more valuable to health and humanitarian teams while ensuring our AI-assisted terminology mapping reflects the realities of resource-constrained health systems worldwide.

Built openly.
Shared with the global health community
All our implementations are open-source. Clinical forms, concept mappings, and data pipelines — built in the open, reusable by the community. View our open-source repositories on GitHub →




Common questions.
Straightforward answers.

Madiro Labs helps humanitarian and public health organizations deploy and operate open-source digital health systems. We cover the full stack: EMR implementation, health data interoperability, clinical terminology standardization, offline field infrastructure, and local team capacity building.
We work globally in humanitarian and low-resource settings — including Iraq, Lebanon, the Democratic Republic of Congo, Eswatini, and Burundi. Our systems are designed for conflict zones, remote clinics, and national-scale health programs.
We work with OpenMRS 3 (EMR), DHIS2 (national health reporting), OpenFn (interoperability layer), OpenConceptLab (clinical terminology), Apache Superset (analytics), and FHIR-native Android apps for community health workers — following OpenHIE architecture.
Yes. We deploy fully offline-first clinical applications with encrypted local storage and automatic sync when connectivity is available. For field operations, we also install solar power and satellite or cellular connectivity infrastructure.
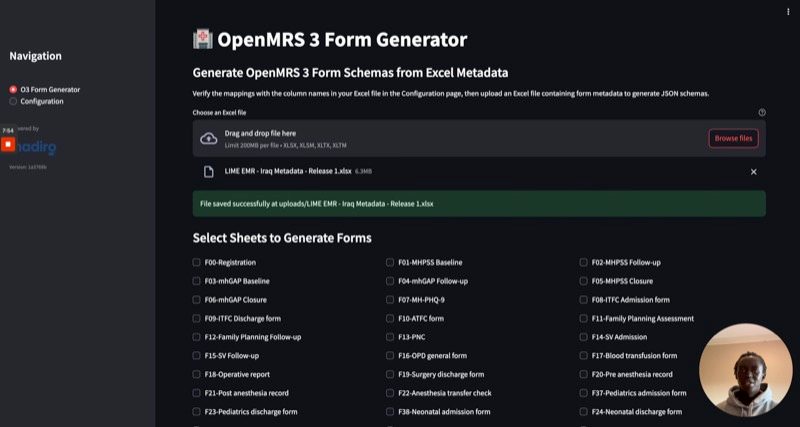
Using our AI-assisted workflow and a library of 70+ reusable forms across 12+ health programs, a new form can be built, terminology-mapped, and deployed in under 5 days. Health programs that previously took months now launch in days.
Every engagement is designed for knowledge transfer. We provide intensive on-site training, co-build with local technical staff, and measure success by your team's independence — not by our ongoing involvement.
Use the contact form on this page to describe your challenge, country context, and existing systems. We respond within 48 hours with an assessment.
Madiro Labs is a registered non-profit. We work on project-based engagements funded through donor grants, organizational budgets, and global health program funding — including co-authoring concept notes and serving as a technical consortium partner on larger proposals. Every surplus is reinvested in the mission. Our pricing is designed for humanitarian and public health contexts, not commercial healthcare markets.
Costs vary significantly depending on scope, geography, and existing infrastructure. A form development sprint may run a few thousand dollars; a full EMR deployment with training and handover typically ranges from $30,000 to $150,000+ depending on scale and duration. We work transparently within grant budgets and can help scope an engagement that fits your available funding.
Every engagement is designed to end with your team in control. We provide a structured handover, training documentation, and a defined post-go-live support window. Beyond that, we offer optional retainer arrangements for organizations that want continued technical advisory. Our goal is your independence, not dependency.
Yes — and we do this regularly. We serve as named technical consortium partners on concept notes, EU calls, USAID programs, and foundation grants. We contribute the technical narrative, logical framework, implementation methodology, and budget architecture for the digital health component. We can co-author or review, depending on your timeline. Use the contact form and select 'Technical Partnership / Consortium' to start a conversation.
Yes. We have in-house research capacity and active academic partnerships. Our work has been published in peer-reviewed journals including Eurosurveillance and BMJ Open. We co-author implementation research, measure health system outcomes, and publish findings in peer-reviewed and grey literature. If you are building a research consortium or seeking a technical partner for an evidence-based program, contact us to discuss co-investigation arrangements.
No. Our AI tools operate exclusively on de-identified configuration data, form schemas, terminology mappings, and documentation — never on identifiable patient records. All AI-assisted workflows are designed to run on local infrastructure or private cloud instances where the data stays in-country. Patient privacy is a non-negotiable constraint in our architecture, not a feature.
Every AI output in our stack is reviewed and approved by a qualified clinician before it enters production. AI assists with drafting — it never autonomously deploys clinical logic. For example, AI-generated clinical forms and terminology mappings go through a structured review cycle with the implementing health team. We document every AI-assisted decision as part of our open-source implementation record, so nothing is a black box.
Built for where
the system breaks down.
We work in humanitarian response, global health, and low-resource settings — not commercial healthcare. We'll tell you straight if we're the right fit.
You're in the right place if…
- You're deploying in fragile, conflict-affected, or climate-exposed settings where standard tools fall short
- You're a Ministry of Health or NGO building systems that local teams will own — not depend on vendors to maintain
- You use or are evaluating open-source tools — OpenMRS, DHIS2, OpenFn, or FHIR-based systems
- You're designing a concept note, grant proposal, or consortium and need a trusted technical partner
Book a 60-min
working session.
We'll map your current stack, identify 2–3 quick wins, and send you a short action memo within 48 hours.
Madiro team combines experts in global health and research with 120+ years of combined experience. Our team has built and deployed open-source health systems directly with MSF, ICRC, and Ministries of Health across 20+ countries.
Offices
Your Interest *